What is abdominal aortic aneurysm (AAA)?
The aorta is the largest artery in your body, and it carries blood away from your heart. Your aorta runs through your chest, where it is called the thoracic aorta. When it reaches your abdomen, it is called the abdominal aorta. The abdominal aorta supplies blood to the bowel, Kidneys and lower part of the body. Just below the abdomen, the aorta splits into two branches that carry blood into each leg.
When a weak area of the abdominal aorta expands or bulges, it is called an abdominal aortic aneurysm (AAA). The pressure from blood flowing through your abdominal aorta can cause a weakened part of the aorta to bulge, much like a balloon. A normal aorta is about 1 inch (or about 2 centimeters) in diameter. However, an AAA can stretch beyond its safety margin. Aneurysms are a health risk because they can burst or rupture. A ruptured aneurysm causes severe internal bleeding, which leads to shock or even death.
AAA rarely causes other serious health problems. Clots or debris form inside the aneurysm and can travel to blood vessels leading to other organs in your body. If one of these blood vessels becomes blocked, it can cause severe pain or even more serious problems, such as limb loss.
Each year, physicians diagnose approximately 200,000 people in the United States and 20,000 annually in Australia with AAA. In USA, almost 15,000 AAA rupture and die each year, but there are also a large number of people who die suddenly with no cause of death which could account for another 15,000. Hence ruptured AAA is a major cause of death in males.
Fortunately, when diagnosed early, endoluminal surgery for AAA is effective and safe. Hence there is a need for all males over 65 years of age to have a simple ultrasound test performed on there abdomen to exclude AAA.
What are the symptoms?
You usually do not feel any symptoms with AAA. However you may experience one or more of the following:
- A pulsing feeling in your abdomen, similar to a heartbeat. This only occurs when the AAA is large.
- Severe, sudden pain in your abdomen or lower back. If this is the case, your aneurysm has burst and you must seek medical help urgently.
- On rare occasions, your feet may develop pain, discoloration, or painful because of material shed from the aneurysm
If your aneurysm bursts, you may suddenly feel intense weakness, dizziness, or pain, and you may eventually lose consciousness. This is a life-threatening situation and you should seek medical attention immediately.
What causes an abdominal aortic aneurysm?
Physicians and researchers are not quite sure what causes AAA. The leading thought is that the aneurysm may be caused by inflammation in the aorta, which may cause its wall to break down. Some researchers believe that this inflammation can be associated with atherosclerosis (also called hardening of the arteries) or risk factors that contribute to atherosclerosis, such as high blood pressure (hypertension). In atherosclerosis fatty deposits, called plaque, build up in an artery. Over time, this buildup causes the artery to narrow, stiffen and possibly weaken.Besides atherosclerosis, other factors that can increase your risk of AAA include:
- Being a man older than 60 years
- Having an immediate relative, such as a mother or brother, who has had AAA
- Having high blood pressure
- Smoking
Your risk of developing AAA increases as you age. AAA is more common in men than in women.
What tests will I need?
Abdominal aortic aneurysms are most often found when a physician is performing an imaging test, such as an ultrasound, for another condition. If your physician suspects that you may have AAA, he or she may recommend one of the following tests:
- Vascular ultrasound for AAA
- Computed tomography angiogram (CTA)
How is an abdominal aortic aneurysm best treated?
Watchful waiting
 "Watchful waiting," means that you will be monitored every 6 - 12 months for signs of changes in the aneurysm. Your doctor may schedule you for regular vascular ultrasound scan to watch the aneurysm. This method is usually used for aneurysms that are smaller than 4.0 centimeters. If you also have high blood pressure, your physician may prescribe blood pressure medication to lower your blood pressure and lower the pressure on the weakened area of the aneurysm. If you smoke, obtain help to stop smoking. An aneurysm will not "go away" by itself. It is extremely important to continue to follow up with your physician as directed because the aneurysm may enlarge to a dangerous size over time and could eventually burst.
"Watchful waiting," means that you will be monitored every 6 - 12 months for signs of changes in the aneurysm. Your doctor may schedule you for regular vascular ultrasound scan to watch the aneurysm. This method is usually used for aneurysms that are smaller than 4.0 centimeters. If you also have high blood pressure, your physician may prescribe blood pressure medication to lower your blood pressure and lower the pressure on the weakened area of the aneurysm. If you smoke, obtain help to stop smoking. An aneurysm will not "go away" by itself. It is extremely important to continue to follow up with your physician as directed because the aneurysm may enlarge to a dangerous size over time and could eventually burst.
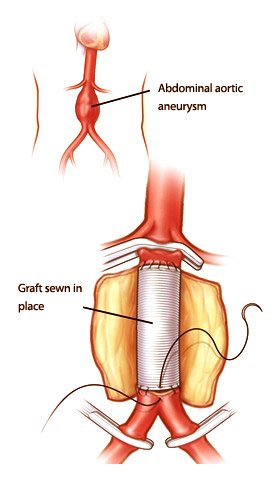
Open surgery - Major open surgery
In this procedure a large incision is made in the abdomen, the bowl is moved to one side and the aneurysm is opened, while the circulation is stopped by clamping above and below. A synthetic dacron graft is sewn into place and when bleeding is controlled the abdomen is closed. This is a major operation which requires a long period of recovery (up to three months). A mortality of approx 5% and major complications. It is not performed now by surgeons that have an understanding of endoluminal grafting. In public hospitals because of cost considerations this procedure may be recommended.
Endovascular stent graft
In the last ten years instead of open aneurysm repair (open surgery), a newer procedure called an endovascular stent graft has become the preferred treatment. Endovascular means that the treatment is performed inside your body using long, thin tubes called catheters that are threaded through your blood vessels. This procedure is less invasive, meaning that your surgeon will need to make a small incision in your groin area through which to thread the catheters. During the procedure, your surgeon will use live x-ray pictures on a video screen to guide a fabric and metal tube, called an endovascular stent graft (or endograft), to the site of the aneurysm. Like the graft in open surgery, the endovascular stent graft also strengthens the aorta. Your recovery time for endovascular stent graft is usually shorter than the open surgery, and your hospital stay may be reduced to 2 to 3 days.
However, this procedure requires more frequent imaging procedures after placement to be sure the graft continues to function properly, and is more likely to require periodic maintenance than the open procedure. In addition, you may not be suitable for a standard graft, since not all patients are candidates for routine endovascular repair because of the extent of the aneurysm, its relationship to the renal (kidney) arteries, or other issues.
A standard graft is suitable for 80% of AAA's and can be readily obtained. A customised graft takes two months to obtain the design, manufacture and sterilisation. It is usually a "fenestrated" graft - this means there are holes in the graft for renal and mesenteric arteries.
With these techniques, it is now possible to treat greater than 90% of AAA using the endoluminal approach. In addition, with graft improvements, reintervention after graft placement is now minimal, but annual surveillance is still required.
If this is the case your AAA will need to be assessed for a customised graft. This is specially tailored to your AAA's anatomy and is more difficult to place.
Dr Alan Bray was involved with the early development of the endoluminal procedure for over ten years. He is a proctor for the Zenith AAA graft, especially for the fenestrated graft.
He is an acknowleged expert in this field, having given many presentations at international meetings on various aspects of this new technique.